Author's disclaimer
The patient-specific details in the narratives below are altered to protect the patinets' confidentiality. Thank you for reading.
Sincerely, Ryan
Labels: Media
posted by Ryan @ 9:28 AM
1 comments
![]()
![]()
A pediatrician named Ryan Phelps from Denison, TX tells tales about his work in Swaziland with the Baylor International Pediatric AIDS Initiative, among other things.
The patient-specific details in the narratives below are altered to protect the patinets' confidentiality. Thank you for reading.
Labels: Media
posted by Ryan @ 9:28 AM
1 comments
![]()
![]()

Please see the link below for this week's Time magazine article about BIPAI. The second link will take you to a related video filmed at the Baylor site in Lesotho.
http://www.time.com/time/magazine/article/0,9171,1562960-2,00.html
http://www.time.com/time/video/2006/pediatric_aids_gorman/Labels: Media
posted by Ryan @ 5:16 PM
0 comments
![]()
![]()

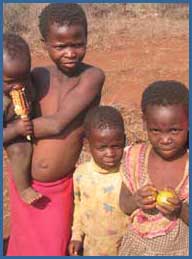
There are around 1,000,000 people living in Swaziland. 500,000 are adults. Up to 200,000 of those adults are infected. Most of those infected are caring for children. 20,000 of those infected need ARVs immediately, or they will soon die of AIDS. The remaining 180,000 adults have an average of around 10 years before they will meet the same fate.
Today, there are 70,000 orphans in Swaziland. In 2010, there will be around 120,000.
120,000 children without adult caregivers.
This is not complicated math, and the dangers of allowing 120,000 parentless, unschooled, unemployed, undernourished, helpless, hopeless children wander a small country are not difficult to calculate either.
In the words of Derek Von Wissel, the Director of Swaziland's National Emergency Response Council on HIV/AIDS (NERCHA), “They will have nothing to lose. They will be rampant. It is a nightmare.”
This is a nightmare we will most certainly want to wake up from. Should we not wake up sooner than 2010?
To do your part, see the following link, or email me for other ideas as to how you might contribute.
www.youngheroes.org.sz/index_home.asp

Labels: Photos and "shorts"
posted by Ryan @ 8:42 AM
1 comments
![]()
![]()

Labels: Patient encounters
posted by Ryan @ 5:56 PM
0 comments
![]()
![]()
The following NY Times article (24 Nov) relates to the entry titled "The deepest cut". Have a look.

Labels: Media
posted by Ryan @ 5:55 PM
1 comments
![]()
![]()


Labels: What am I up to?
posted by Ryan @ 2:31 PM
0 comments
![]()
![]()

Labels: Patient encounters
posted by Ryan @ 1:17 PM
2 comments
![]()
![]()

posted by Ryan @ 12:35 PM
0 comments
![]()
![]()
Suppose you were a fly on the wall...
Doctor’s Meeting Minutes (DRAFT), 24 November, 2006
(Respectfully submitted by Ryan. Actionable items in red. Contact me with additions/corrections.)
1) Patient flow log (Delouis)
· Reviewed purpose of log, which we will use for 2-3 days to gather info on pt flow and complexity of visits. Translators to fill out with MD help as needed.
· Also logging lab entry time to measure how many MD-hours being used.
· We are doing both of these logs to improve efficiency and to build argument to hire digitizing staff to protect MD time. Discussion ensued.
2) Outreach updates (Dewey et al.)
· What is going on, in brief? Are folks happy or wanting to rotate?
· Piggs Peak
- Dave and Dan D. in PP, getting to know folks and doing bit of everything.
- There are 5 docs there, but PMTCT strategies are high yield investment opps for our docs (little VCT, with 50% or more HIV+ but poor f/u).
· Shumwula/Lomahasha/Good Shepard (Gretchen and Helga)
- Gretchen and Helga happy to have other docs come with them.
- The perspective from being “out in the field” very valuable.
- Gretchen recommends grant-writing over holidays to try to ensure some inflow, esp. for transport. (UNICEF a “maybe” at this point.)
· Matsangeni Govt Hlth Center (Sach)
- Many challenges, esp. in peds and PMTCT. (Eg: Cotrim/MVTs often not available.)
- Still, have made great strides in short time, building inroads and demonstrating partnership and support.
· Mbabane Govt. Hosp (Nanda)
- This has been Nanda’s site for 3 months, and she sees positive changes with her persistent presence. (Eg: Malnutrition protocol starting to work.)
· COE (Amy, Julia, Eric, Ryan, Johanna, and others):
- All generally happy at COE, but little protected time for other projects.
- Working on pt flow.
3) Protocol committee
· Diarrhea (Helga)
- Reviewed “Diarrhea SOP” draft, derived from Uganda SOP.
- Reviewed zinc, vit A, antimicrobials, and antidiarrheal data, in brief.
- Plan to look over diarrhea SOP and discuss/edit next week.
- Need for water hygiene handout and rehydration SOP.
· Adult ARVs (Eileen)
- AZT vs D4T for adult is a question that freq comes up
- Proposes we shift from D4T to AZT for new ARV pts unless good reason not to
- Also cited 2 recent studies from Uganda and SA (see Eileen for refs)
- Cut-off for anemia in adults <>
Labels: Photos and "shorts"
posted by Ryan @ 12:22 PM
1 comments
![]()
![]()






Labels: Other stories
posted by Ryan @ 7:52 PM
0 comments
![]()
![]()

Labels: Media
posted by Ryan @ 9:01 PM
0 comments
![]()
![]()

Labels: Photos and "shorts"
posted by Ryan @ 7:57 PM
0 comments
![]()
![]()

Labels: What am I up to?
posted by Ryan @ 9:47 AM
0 comments
![]()
![]()


Labels: Photos and "shorts"
posted by Ryan @ 5:15 PM
1 comments
![]()
![]()


Labels: Media
posted by Ryan @ 4:50 PM
0 comments
![]()
![]()

Labels: Photos and "shorts"
posted by Ryan @ 3:41 PM
0 comments
![]()
![]()

Labels: Photos and "shorts"
posted by Ryan @ 3:13 PM
1 comments
![]()
![]()
“Look, the moon is full,” said one of the silhouettes as we wandered down the shore of Lake Malawi.




Labels: Photos and "shorts"
posted by Ryan @ 12:34 PM
0 comments
![]()
![]()




Labels: Photos and "shorts"
posted by Ryan @ 9:39 AM
0 comments
![]()
![]()
Labels: Photos and "shorts"
posted by Ryan @ 11:47 PM
0 comments
![]()
![]()
Some of you have asked me to post intermittent "informational" blogs about my day-to-day, and so I begin with this past week, which I spent outside of the kingdom of Swaziland in the country known as "the warm heart of Africa"--Malawi.



Labels: What am I up to?
posted by Ryan @ 7:51 PM
0 comments
![]()
![]()




Labels: Photos and "shorts"
posted by Ryan @ 4:21 PM
0 comments
![]()
![]()




Labels: Photos and "shorts"
posted by Ryan @ 3:32 PM
0 comments
![]()
![]()

