Swazi sunset

posted by Ryan @ 12:52 PM
0 comments
![]()
![]()
A pediatrician named Ryan Phelps from Denison, TX tells tales about his work in Swaziland with the Baylor International Pediatric AIDS Initiative, among other things.

Labels: Patient encounters
posted by Ryan @ 2:29 PM
0 comments
![]()
![]()




Labels: Photos and "shorts"
posted by Ryan @ 4:03 PM
0 comments
![]()
![]()
Labels: Media
posted by Ryan @ 3:07 PM
0 comments
![]()
![]()
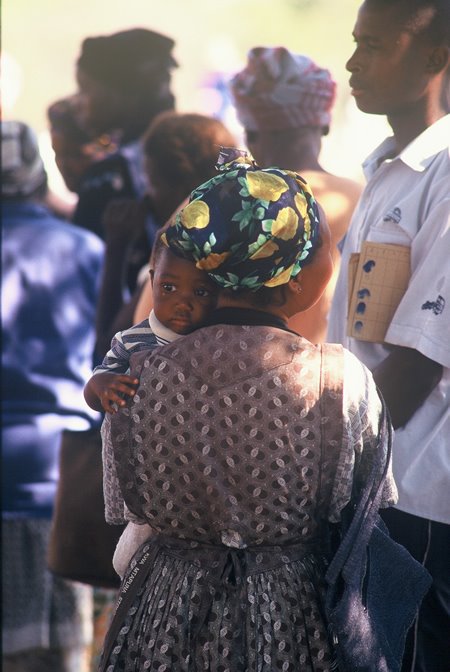
 (Swazi grandmother with children.)
(Swazi grandmother with children.)Children are ticklish, even those close to death. Benele certainly was.
He walked in the room with his grandmother. He peered at me in manner that I have become accustomed to since arriving in Swaziland. It was not the look of fear or anxiety that pediatricians typically inspire. It was that of a child trying to hide the amusement inspired by having such a strange-looking doctor.
The grandmother’s eyes communicated something different. In her gaze was that uneasiness that one feels when one does not know what to make of a strange-looking doctor. Noticing this, I put down Benele’s chart and explained to her that I had traveled from the United States to help take care of children such as Benele because I want him to grow up and grow strong. She answered me with the same, skeptical look.
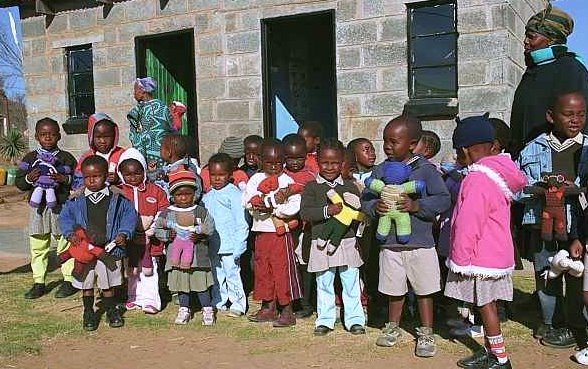
If HIV is pulling Swaziland apart, then Swazi grandmothers are one of society’s most sticky glues. When mothers get sick or die, the children go to the grandmother (called “gogo” in SiSwati). A gogo can in this way accumulate over a dozen dependents. These women are a reservoir of wisdom, dedication, and surrogate motherhood in this kingdom’s troubled times.
If a Swazi household is being held together in a country where over 40% are HIV infected, it is because of the gogo. This child was alive because of the efforts of this gogo. Benele’s chart told the story of a dying, orphaned child with but one advocate. I wanted to join forces, but I was going nowhere if she did not trust me.
I asked the gogo what her name was. She told me (it was long and difficult to pronounce) and I repeated it back to her. She smiled and looked at the ground and then at the translator whom she did not need as her English was excellent. I said that I was sorry that I could not say it well but that I was studying her language and that next time I met her I would say her name well and then greet her, for I knew too little SiSwati to do either at that moment.
She smiled, paused, and said, “With pronunciation like that, you will be speaking SiSwati very soon.” I thanked her for the compliment, and she smiled, her eyes meeting mine and staying there. After a few seconds, she said something to the interpreter and they both laughed. She said, in perfect English, that she was happy that I was coming here to see Benele and learn SiSwati. A partnership was kindled, and I turned toward my 8 year-old patient, who needed both of us badly.
For nearly nine years, Benele’s body had been fighting HIV. The disease increases caloric expenditure and nausea and decreases energy and appetite, so it was no surprise that his body weighed just over 30 lbs. After shaking the child’s diminutive hand, I leafed through his chart. He was started on ARVs at the government hospital well over a year ago, but his CD4 count never improved. He had not gained weight for nearly a year. Each page of his thick medical chart was riddled with the names of opportunistic infections. In more recent visits, one could find words like “possible resistance” and “despite first-line therapy”.
Benele’s medicines were not working, and this is uncommon in a child receiving appropriate first-line antiretroviral. There are many potential reasons for Benele’s predicament. HIV, despite being infinitesimally small, is very clever. It is constantly reinventing itself, forever learning. HIV inherently replicates itself with a high error rate, amassing offspring with millions of mutations. Those whose mutations allow them to survive whatever the human body or medical science throws at them pass that mutation on. This process usually takes many years. But, if HIV gets lucky, or a patient misses multiple doses, it can occur rapidly.
In other words, HIV makes Darwinism look easy. For this reason, it is one of humankind’s most venerable modern enemies. For this reason, Benele’s HIV had found a way to survive the highly active antiretroviral therapy that he had been on for nearly two years, and AIDS was in the process of killing him.
Benele’s arms were like broom handles, his abdomen like an overfilled duffle bag, his large spleen and liver accentuating his frail limbs. As my eyes were examining Benele’s tiny, distorted body, his eyes were examining me. He seemed to have a minor scabies infection, but it was difficult to be certain as his body is not able to mount a normal immune response to the invading mite. I pulled out my stethoscope. He was still gazing at me. His pneumonia, diagnosed at his previous visit, was getting better on his current antibiotics, it seemed. His lungs still sounded horrible, but he was breathing with less effort, a practical and reassuring improvement. I looked into his eyes and placed my hands below my own chin show him that I was going to do the same to him. Children with HIV/AIDS have very abnormal lymph nodes, and this is a common place to feel for them. After my gesture, he lifted is chin, and I reach for him.
I do not know how a child can laugh so loud with such a broken body.
How do his eyes still shine so?
How did I get to be so lucky to have the privilege of being in the same room with this sick, beautiful, ticklish boy?
I charted my exam findings and sent Benele to the pharmacy to retrieve his second-line HIV therapy, the medicines that I hope would reduce his viral load, increase his CD4 count, and renew his body’s innate ability to fight infection. The new drugs are designed to attack Benele’s HIV by a different mechanism than the initial regimen, and his chances of improvement are good.
“Siyabonga”, gogo said as she left the exam room. This was a word I knew. It meant “thank you”. I wanted to stop her and tell her how much I admired her. I wanted to explain that helping her ticklish grandson live to grow up to be a strong man made me feel proud and alive. I wanted to tell her that hearing him laugh filled my heart.
Instead, I said “You’re welcome,” for I could not find the words, and the waiting room was full.
Labels: Patient encounters
posted by Ryan @ 1:54 PM
1 comments
![]()
![]()




Labels: Other stories
posted by Ryan @ 5:21 PM
0 comments
![]()
![]()
“I am one confused citizen,” she said, slowly shaking her head. “Sometimes I just want to lie down and die with my baby.”
These were the words of my first patient in Africa. Her name was Thembela. She was HIV infected, as was my second patient in Africa, the baby she cradled in her arms. The baby swayed side to side in synchrony with the dejected mother’s bowed head. The baby was 13 months old, and already demonstrated signs and symptoms of acquired immunodeficiency syndrome, or AIDS.
Children acquire HIV during birth or while breastfeeding, with rare exception. If an HIV infected child’s fortune can be compared to a game of cards, the child’s hand is a 2-7, off-suit. If these two cards are placed face-down in front of you, you do not bet on winning.
This child was not winning.
Thembela’s hand was no better. She lived in a home where there where certain words that were never spoken, a home where certain topics of conversation were taboo, a home where 15 or so others lived, mostly in-laws. To bring up these unspeakable things was to risk being banished from the home altogether.
In Swaziland, a diagnosis of HIV brings with it great stigma. If you declare your status, you immediately embody everyone’s worst fear. You become a reminder to all who see you that they too could be dying and not even know it. Such reminders were forbidden in Thambela’s home.
The mother explained all of this to me, then looked at me blankly.
Texas Hold-em is a variation of 5 card draw. If you have not heard of it, you either do not have cable or have cable and have never surfed the second-tier sports channels. I like it because anybody can win. It is a game where seeming average makes you above average, and where almost every winner looks average. It is a game that reminds me of home.
My extended family stretches from just south of the Oklahoma border to Houston. When we get together, we play Texas Hold-em. We play for money, trophies, bragging rights, and pride. We play hard and late into the night. I have been here in Swaziland for a few weeks now, and I think fondly of those late nights. I think of the laughter, the companionship, the Shiner Bock, and what it means to be home, surrounded by loved ones.
Looking into my very first patient’s expressionless face, I realized that, for her, being home meant lying. It meant playing a losing hand as well as she could. It meant keeping a straight face while watching everything slip away. It meant bluffing until death.
“I am one confused citizen,” she said, slowly shaking her head.
I was one confused doctor. This woman could not take my medicines home, and she could not be seen taking them or giving them to her baby. She could not tell anyone she had ever been to our “HIV clinic”, and she could never allow anyone to see that she and her baby were getting more and more sick, that they were dying.
If she did this, she would become a Swazi woman with HIV, an HIV-positive child, and no family or other financial support. She would be alone.
We spoke of her alternatives. We spoke of her strengths. We scheduled her next visit, when she would bring with her an ally from her community, in secret if necessary, to learn about the medicines and how to give them. With this support, Thembela and her child are much more likely to be able to properly store and dose the medicines without being discovered.
“You do not have to do this alone,” I said. “Your baby is going to grow up, and she will need you to take care of her.”
Three weeks later, Thembela has a thriving business selling chicken and rice lunches in front of our clinic. She sells a few dozen such meals daily, for six Lilanginis each (approximately 90 cents). She is planning to use the profits to rent a room down the road from the clinic, where she will cook lunches, raise her child, and keep her ARVs.
I eat her lunch every day. Some days the chicken and rice come with greens and potatoes, some days beetroot, others spinach. Delicious.
“Remember me?” she asked when I saw here outside of the exam room for the first time. “I am your first patient.” I said that I remembered very well, searching my pockets for coins. “I am saving the life of my child,” she said, smiling.
I smiled back.
Well played, Thembela.
Labels: Patient encounters
posted by Ryan @ 10:50 AM
0 comments
![]()
![]()
So, here I am.
The following paragraphs are from the desk of Ryan Phelps, a pediatrician from
On August 18th, 2006, I boarded a plane in
Swaziland has the highest HIV prevalence in the world. Swaziland has a king, and he has many wives (in excess of a baker’s dozen). Swaziland has around a million Swazi’s living in it, and the landmass is approximately the size of New Jersey, though I wish I knew of another place about the size of New Jersey to avoid having to make this particular comparison. I make no apologies for the bakery analogy, however, for the king only marries once his chosen mate has a bun in the oven. What an immaculate concept.
The many-ovened king is a beloved man here, lording over a kingdom steeped in tradition, including culinary ones. He has inherited Swazi law and custom and the coveted duty of perpetuating it and (perhaps) benefiting from it. He does not cook. All Swazi men, king down to humblest pawn, make (and occasionally break) the rules around here. I say this without judgment, for I am ill-qualified (and otherwise reluctant) to charge or indict my hosts. It is very early spring here, and the weather is warming. When the chicks that hatch in a few weeks can be found within the small Styrofoam containers being sold at the local "Chicken Lickin", I will write a more seasoned editorial. Until then, I sincerely mean it when I say that I appreciate the kingdom of Swaziland granting me the opportunity to live and work here. In a world where few own a passport or ride a motorized vehicle, my doing both with a monarch’s blessing is a rare privilege, a trifecta of sorts.
My privileged voyage to Swaziland has two primary purposes: to help treat children (and adults) with HIV and teach other health care providers to do the same. I aim to do both to the best of my ability. As I do this, I plan to draft what one might call “field narratives” to share my experiences. I will do this with the best of this novice writer’s ability also. All efforts undertaken by amateurs (including amateur writers) must come with a disclaimer, and here is mine: I have never kept much of a diary nor written anything of import. For that matter, I have yet to even create an unimportant and yet entertaining read. Knowing as little as I do, however, I can assure you, the reader, that though I have only the most basic idea of why I am here, you will be among the first to know of my successes, failures, and lessons learned. Even if I am unable to accompany my observations with insight, I pledge to record my observations carefully, offering a sort of looking glass into this part of the world.
The near and distant future of Swaziland, including the small role I am to play within it, is uncertain. At present, the worst of the modern-day plagues surrounds me. It is not like previous plagues, for which death was the only option. This disease can be treated. Still, millions die. This is why this ill-qualified writer writes; I believe strongly in what we are doing here.
My faraway backdrop is Swaziland’s capital, Mbabane, a clean town of approximately 80,000 perched above a large valley and among small stony mountains. I do not know the type of rock, but they are a sandy-beige and their effect is most inviting. It is the type of terrain that looks good on the cover of magazines that sell high-tech, expensive outdoor gear. For this and other reasons, my impression of Mbabane is that it looks (abounding natural beauty) and feels (crisp, sunny early spring days and friendly people) like a place where one would not mind living. Of course, I am told that the honeymoon when changing continents and cultures can last six months, so my descriptors may change after I have bedding here for a longer spell.
Traditional Swazi village
I live in a large, comfortable house with a sheltered, suburban feel and sufficient bedding for any potential guests. Hot water and electricity—yes, usually. Central air—no. My yard has an avocado tree and is surrounded by “bluegum” trees and pines. The avocados fell to the ground and rotted just before my arrival. Darn. Within the nearby pines are dozens of pendulous, tear-shaped nests belonging to small weaver birds that I have yet to google and speciate (Swazi internet is glacial, and yes, the verb ‘google’ is now officially part of Webster’s). The weaver nests look a bit like avocadoes but are well beyond reach, firmly attached, and, as far as I can see, inedible.
I guess I will have to wait around a while for the free avocadoes. I need to cultivate an onion, tomato, and jalapeño patch so that I can make guacamole when that time comes. Of course, I cannot make margaritas without a lime tree and agave cactus plant. It seems as though I have a lot of gardening to do to minimize homesickness.
Though Tex-Mex is but a dream, Mbabane has similarities to Denison, Texas. At night, in my back yard, frogs croak and crickets chirp. Occasional woodpeckers peck. Cars are rarely heard.
Unfortunately, there is a very un-Texan, sickly rooster nearby that occasionally calls out to the local henhouse, though the call is more like a cough or wretch than a cock-a-doodle-doo. Actually, when he crows in the middle of the night, the sound closely resembles that a belch would make if one where being choked while belching. I hope that the hens share my opinion, for should this rooster father a dozen little belchers, my community’s charm (and similarity to rural Texas) would be in grave jeopardy.
My home does not resemble that of most Swazi homes, which are organized within a traditional rural patriarchic, patrilineal village. This ex-patriot will have to defer on the definitions of these anthropological categories, for I am not an anthropologist.
The streets of Mbabane are mostly paved (and mostly free from trash) as are the main highways heading west (to Johannesburg), south (to Durban and Capetown), and east (to Maputo). The town center is lively and equipped with shops selling the familiar (KFC, Woolworth’s, Shell) and the unfamiliar (specific examples require familiarity). All that one truly needs, and more, can be found in Mbabane.
I navigate my new town on the left side of the road in a car with its steering wheel on the right. I am allowed to take a left on a red light. All of this frightens me, so I bought a mountain bike for my commute to work (1.5mi). Besides, there are all of those alluring mountains on all sides, so I had to gear up.
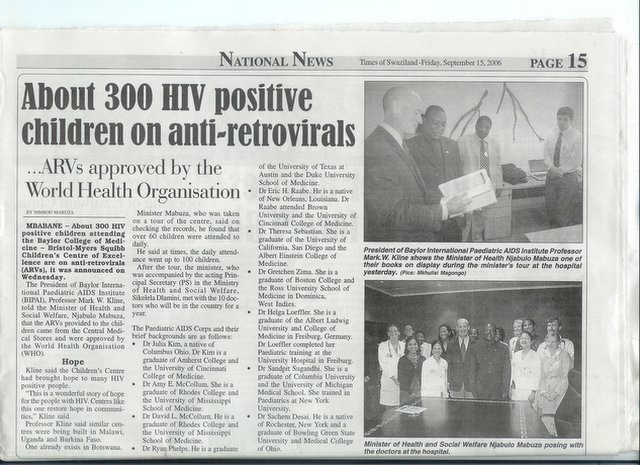
The clinic where I work is called the Baylor College of Medicine - Bristol-Myers Squibb Children’s Clinical Centre of Excellence, Swaziland, or “COE” for short. It is a spacious, newly-constructed building where children and parents can receive HIV testing and treatment. It walls are adorned with Swazi handicrafts, cultural garb, and various local photos. One hanging reed mat has woven into it the words, “Feel at home”, and it is indeed a cozy, welcoming place. Within these walls, a small number (in the hundreds) of children and family members receive medicines that have the potential to allow them to grow old though infected with HIV. My job is to try to increase this number (with a goal of >1,000 patients on antiretroviral treatment within a year) and expand pediatric HIV services in other parts of the country.
A child dies of HIV/AIDS every 60 seconds. This is disease that destroys children, families, and continents. Worse still, it destroys hope. It is a disease that leaves me feeling under-qualified despite spending my teens and twenties pursuing qualifications. Though HIV is an intimidating virus, excellent treatment exists. A very small proportion of Africans with HIV receive this treatment.
There is a catchy saying here. It goes something like: “Let’s put one and one together and see if we get two.” I have no delusions that I am going to save the world, but putting effective, available medicines and dying human beings together adds up. Failing to do so does not. So, here I am.
Labels: Other stories
posted by Ryan @ 4:36 PM
2 comments
![]()
![]()



{kind=link}
{kind=link}
{kind=link}
{kind=link}